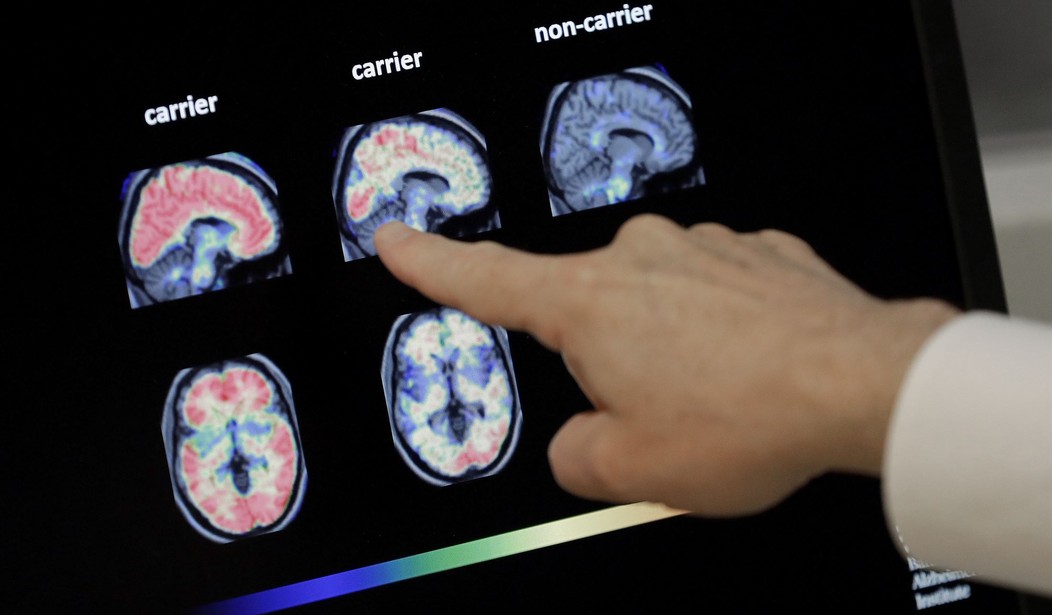
Yesterday the NY Times published an excerpt from a book about a new approach to treating people with serious psychoses, specifically people who routinely hear voices or see images. The standard approach to these cases is diagnosis and medication with some combination of anti-psychotic drugs. But as the excerpt describes in detail, those drugs don’t always work and even when they do they can have serious side effects.
So the bulk of this piece is about a new approach that is being tried in a few places around the world. It could probably be described as a psychotherapy approach rather than a psychiatric approach. And it focuses on one woman who has made that transition after a youth and adolescence filled with voices and medication.
Caroline Mazel-Carlton began hearing voices when she was in day care. Mornings, by the time she was in middle school, a bowl of oatmeal awaited her for breakfast next to a white saucer of colorful pills. Her voices remained vibrant. They weren’t within her head; they spoke and screamed from outside her skull. They belonged to beings she could not see.
The voice who had been with her longest warned of catastrophes coming for her family in Zionsville, a town north of Indianapolis, calamities tied in some unspecified way to TV images from the gulf war: fighter planes, flashes in the sky, explosions on the ground, luminous and all-consuming. A woman’s voice castigated her at school, telling her that her clothes smelled and that she had better keep her hand down, no matter that she knew the answers to the teacher’s questions. Another voice tracked her every move, its tone faintly mocking. “She’s getting out of bed now; oh, she’s walking down the hall now.”
Things don’t improve from there. Mazel-Carlton gets into college thanks to a perfect score on the verbal portion of the SAT, but she winds up using drugs in addition to her prescriptions to try to self-medicate. Eventually, the turning point in this story is when she decides to flush her medications down the toilet:
Her third arrest was for stealing electronics to trade for drugs. It may only have been the wherewithal of her parents, both lawyers, that spared her a criminal sentence. She was sent to a high-end locked ward in the outskirts of Houston and then to a psychiatric farm in the foothills of the Appalachian Mountains, where, after dutifully earning the privilege of not taking her pills under the vigilant eye of a nurse, she decided to quit all her medications. The choice was impulsive but not irrational. She felt calmer at the farm, shoveling out sheep stalls and ministering to the chapped hooves of a runt donkey. And she could no longer bear the drugs’ futility and harm. She did no tapering. She flushed the drugs down the toilet morning by morning and evening by evening, careful that if anyone checked her med case they would find the right number of pills remaining.
And from there she wound up in Massachusetts as a mental health peer-support specialist, basically someone who could try to relate to patients with serious mental problems because she’d been through it herself. And there she began a program of peer supported modeled partly after Alcoholics Anonymous called the Hearing Voices Network:
The groups, with no clinicians in the room, gathered on secondhand chairs and sofas in humble spaces rented by the alliance. What psychiatry terms psychosis, the Hearing Voices Movement refers to as nonconsensus realities, and a bedrock faith of the movement is that filling a room with talk of phantasms will not infuse them with more vivid life or grant them more unshakable power. Instead, partly by lifting the pressure of secrecy and diminishing the feeling of deviance, the talk will loosen the hold of hallucinations and, crucially, the grip of isolation.
Mazel-Carlton also worked as a sometime staff member at Afiya house, a temporary residence run by the alliance as an alternative to locked wards. The people who stay at Afiya are in dire need; many are not only in mental disarray but also homeless. Many are suicidal. There are no clinicians on staff, no security personnel, only people who know such desperation firsthand. In the living room, a homemade banner declares: “Holding multiple truths. Knowing that everyone has their own accurate view of the way things are.”
While the group meetings may be partly based on AA, they don’t hold to the most fundamental concept of AA, that the goal of all the openness and sharing and connection to other alcoholics is to help people learn to stay off alcohol so they can live healthy, productive lives. The HVN approach seems to be anti-medication but can’t promise a normal life. Instead it has adopted another philosophy which comes directly from the trans community, i.e. everyone should learn to accept people as they are, including people who hear voices all day:
When she was on the psych ward in Houston in her early 20s, or at the Appalachian farm or the Asheville group home, Mazel-Carlton concealed her voices, and until then at the alliance she hadn’t confided their intensity. But somehow Afiya inspired sharing, though the house had no group sessions and no formal methods. An atmosphere without judgment pulled people into revealing conversations. In a basement den, by the hovering blues and golds of a large fish tank, she talked with a gender-nonbinary person about how they each longed to be completely open about themselves, and yearned to live as examples for other people, but also “about how much that can cost, about how there’s a lot of cruelty in the world.”
The excerpt focuses a lot on the failure of medication and only gradually introduces what this new approach might look like in practice but by the end it does put forward an example that struck me as worrisome. It comes as Mazel-Carlton is counseling the parent of an adult child whose son has been living on the street and believes he is a “like a savior.”
The woman’s grown son believed he was taking directions from God. In the recent past, he had been hospitalized, suicidal, homeless. “He thinks he’s kind of like a savior,” she told Mazel-Carlton. His ever-changing plans terrified her. “I need to know how to talk to him. I don’t want to say the wrong thing. I’m trying to just be there, to be empathetic.”…
“I think it’s good that you don’t go there,” Mazel-Carlton said. “Pharmaceuticals are easily accessible — he knows that. He knows he can make that choice anytime. When a mom brings up medication, it can sound like, I don’t like the way you are. Like, the way you are makes me uncomfortable.”
“I’m freaking out.”
“As adults, the moments when we feel that our parents trust us — that’s the lottery-like feeling,” Mazel-Carlton said.
“To let him be who he is,” the mother said. “Not to get in his face. I’m really working on it.”
So this is someone who has been living on the street and thinks he’s, basically, Jesus and the advice is to accept him as who he is? But what does that mean in this case? The whole issue with psychosis like this is that he’s really not who he thinks he is. He’s not a savior he’s a homeless person with mental problems. I don’t want to just mock this approach, which may have some advantages in some cases, but in this case it’s the equivalent of someone announcing “my pronouns are ‘I am’ and ‘Son of Man'” and asking the rest of us to accept that as the healthiest possible outcome even as this person lives on the street.
This approach is said to be picking up steam in a few place worldwide but what would it mean for all of the mentally ill people currently living on our streets? Does it mean we need to accept them for who they are even if who they are is raving drug addicts who steal to support their habits? Maybe this advice makes some sense for parents of these struggling people who have to maintain a personal relationship with them but I don’t think it makes sense for society as a whole to adopt this approach.
As is often the case, there were some saner voices in the comments.
You haven’t truly lived until you have been physically threatened by a psychotic person in crisis, or heard a psychotic client calmly describe killing the family pets.
Tell me how to deal with those things, and I will be more open to hearing about not treating any symptoms except insomnia.
I didn’t hear that any of these people are working or functioning productively in any way. Roller skating successfully isn’t supporting yourself. Neither is playing the cello. Being so distracted that you can’t bathe or do laundry isn’t moving anyone forward.
I treated a woman who told our intake nurse that she looked like a lion. The nurse had a head full of curly blond hair. Made sense. This woman was so swamped with thoughts and sounds she could not care for her body and could not function in any meaningful way. Allowing her to go out there and not function doesn’t seem to be the kind approach.
That’s the most upvoted comment and here’s the #2 comment:
One of the primary criteria for diagnosing a mental health disorder is functional impairment. If the hallucinations cause no serious functional impairment, it is reasonable to not prescribe anti psychotics.
However, for many, they are crippling. I once saw a 21 year old man in the emergency department who spontaneously attempted to jump from a 4th floor apartment window to his death because he saw his family burning to death in fire and heard a voice commanding him to jump. For so many, anti-psychotic drugs have been literally life-saving.
This author haphazardly criticizes modern biological psychiatry without recognizing the significant benefits it has provided to patients. Conjuring up a new term “nonconsensus realities” only obscures an important aspect of the disease, namely perception of something that is not there.
Comment #3 references Michelle Go who was pushed onto the tracks in front of a subway train in January by a homeless man with a history of mental problems:
Michelle Go, Tim McClean, and Rosalind Junor were murdered by unmedicated schizophrenics because of the “voices in their head.” As a physician, I find this article dangerous, and to pretend otherwise is extremely disingenuous. Cherry picking your sources does not make for an informed viewpoint.
Maybe there’s something positive in the Hearing Voices Network for some individuals but I can see a lot of potential downsides to this approach as well. I hope this trend doesn’t lead to an even less effective approach to homeless people with mental problems than the one we have now.





Join the conversation as a VIP Member