
Why would they conceivably deny a request from local doctors to test a patient whose symptoms were suspicious? It can’t be that they’re overburdened, I hope. The United States had tested a grand total of … 445 people as of Tuesday, fewer than a single Canadian province has.
But it also doesn’t make sense to me that they’d ignore possible transmission at this point purely because the patient himself hadn’t traveled to China recently or knowingly been in contact with another coronavirus patient. The great fear, the entire reason for yesterday’s White House press conference, is that doctors expect “community spread” of COVID-19 to begin within the United States soon, if it hasn’t already. That is, we’re probably already at the point where the genie is out of the bottle and being transmitted between people who have no direct contact with Wuhan or anyone who’s been in contact with someone who’s been overseas recently.
So why would the CDC have declined to test someone who was showing symptoms, knowing that even a single oversight risks further transmission from that patient to those around them?
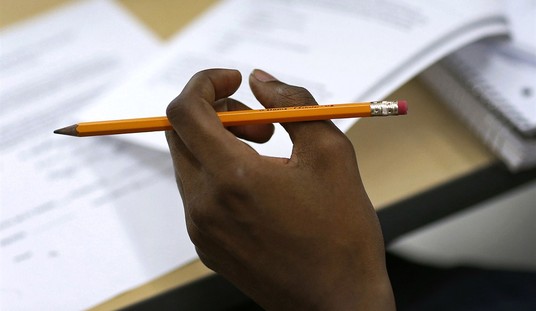
Doctors at the University of California, Davis Medical Center considered the novel pathogen a possible diagnosis when the patient was first admitted last week…
The C.D.C. has restricted testing to patients who either traveled to China recently or who know they had contact with someone infected with the coronavirus…
“Upon admission, our team asked public health officials if this case could be Covid-19,” the letter said. The medical center requested testing from the C.D.C. “Since the patient did not fit the existing C.D.C. criteria for Covid-19, a test was not immediately administered. U.C. Davis Health does not control the testing process.”
The patient was already on a ventilator upon arrival, after being transferred from another hospital in northern California. According to an email sent by UC-Davis officials, he was admitted last Tuesday and went untested until Sunday. Hospital staff took precautions against “droplet contact,” suspecting that the patient had a viral condition, which was hopefully that was sufficient to protect them from coronavirus per the latest CDC guidelines about transmission. As for what precautions were taken by staff at the original hospital, before the patient was transferred, God only knows.
You may be wondering, “Why did the UC-Davis doctors need to wait for the CDC to run this test instead of farming it out to a local lab sooner?” The answer is that the initial test kit that the CDC sent out to U.S. labs had some sort of unspecified defect involving one of the compounds used to detect COVID-19, leading to inconclusive results in around half the labs that used it. That’s why testing here has been so slow. They’re working on an updated test but in the meantime local health officials are desperate:
The nation’s public health laboratories, exasperated by the malfunctioning tests in the face of a global public health emergency, have taken the unusual step of appealing to the Food and Drug Administration for permission to develop and use their own tests. In Hawaii, authorities are so alarmed about the lack of testing ability that they requested permission from the CDC to use tests from Japan. A medical director at a hospital laboratory in Boston is developing an in-house test, but is frustrated that his laboratory won’t be able to use it without going through an onerous and time-consuming review process, even if demand surges.
I wonder what the death toll from red tape will be when this is over.
It remains possible that the UC-Davis patient *isn’t* a victim of “community spread”: Solano County, where the patient is from, also happens to be home to Travis AFB, which is where Americans who were traveling in China and on the Diamond Princess cruise ship are being kept in quarantine. Quite a coincidence. Some of those Americans have since been released. Maybe they were let go too early, when they were asymptomatic but not yet truly cured, and then had glancing contact with the UC-Davis patient among the general population. (Or maybe community spread is happening right now but, for the moment, is still very localized.) There are reports this morning that a coronavirus patient in Japan had exactly this problem: She experienced symptoms, was diagnosed with the illness, was treated and “cured,” and then … got sick again. The fact that asymptomatic patients can spread the disease is frightening enough; imagine if “cured” patients aren’t truly cured, or enjoy no immunity boost after recovery that reduces their chances of being reinfected.
How long should patients be quarantined if we can’t tell when someone is genuinely cured? In a totalitarian state like China, northern California might already be on lockdown as a precaution to limit community spread. How will the United States handle a situation in which the disease is momentarily spreading in a small-ish but highly populated region?
But maybe that’s silly to ask. If we’re hardly even testing for the disease yet, it’s possible that community spread has already been going on for several weeks “disguised” as flu cases. The good news is that, as of 12 days ago, cases of the “flu” weren’t surging. If there were an as-yet undetected spread in coronavirus here, we’d expect to see “flu” numbers surprisingly beginning to rise, I assume. According to a Chinese study, more than 80 percent of coronavirus cases aren’t severe, which is good news in the sense that this isn’t the apocalypse but not so good in that it means more asymptomatic carriers, which means a wider spread. Even a “mild” disease will generate a giant body count if it’s super-infectious.




Join the conversation as a VIP Member