What if I told you that Anthony Fauci knew all along that the COVID vaccine could not possibly prevent either infection with or transmission of COVID?
Not surprised? Neither am I.
Now, what if I told you he just published a paper in a peer-reviewed journal admitting that fact, and calling for new types of vaccines to deal with the problem?
Now that is a bit of a surprise and exactly the opposite of what he told everybody during the push to get everybody vaccinated.
Fauci lied, and now he is admitting it. In writing. In a peer-reviewed journal.
To be clear, Fauci is not claiming that the vaccines were utterly worthless. He still maintains that in certain specific cases–atypical, but the ones that generally kill you–the vaccines serve as a sort of pre-treatment. Not a great one, but a somewhat effective one. But he flat out admits that the claims about the vaccine possibly preventing infection and transmission are simply bogus and always were.
No, I am not exaggerating. He even admits that flu vaccines would never meet the standard to pass muster for use if they were for any other virus. Fascinating. And hardly how they are advertised.
Here’s the abstract of the piece published in Cell, a highly prestigious journal.
Viruses that replicate in the human respiratory mucosa without infecting systemically, including influenza A, SARS-CoV-2, endemic coronaviruses, RSV, and many other “common cold” viruses, cause significant mortality and morbidity and are important public health concerns. Because these viruses generally do not elicit complete and durable protective immunity by themselves, they have not to date been effectively controlled by licensed or experimental vaccines. In this review, we examine challenges that have impeded development of effective mucosal respiratory vaccines, emphasizing that all of these viruses replicate extremely rapidly in the surface epithelium and are quickly transmitted to other hosts, within a narrow window of time before adaptive immune responses are fully marshaled. We discuss possible approaches to developing next-generation vaccines against these viruses, in consideration of several variables such as vaccine antigen configuration, dose and adjuventation, route and timing of vaccination, vaccine boosting, adjunctive therapies, and options for public health vaccination polices.
We haven’t gotten to the (not so) good part yet, but the bolded sentences tell you why these vaccines don’t work as advertised: the vaccines are delivered intramuscularly (you get a shot), which is intended to stimulate a systemic immunological response. You develop antibodies that circulate in the bloodstream.
But respiratory viruses do not generally enter the bloodstream, and when they do they are far past the point of infecting you and being passed along to others. You breathe them in, they replicate quickly, get expelled to infect others, and then may or may not enter the rest of the body. There are other types of viruses that infect you through your respiratory system that have their major impacts systemically, and vaccines can work against them. But for viruses like RSV, Influenza, and COVID-19 this is rarely the case.
This is why you can get COVID while vaccinated, and why when you are more likely to not get as ill if the virus becomes systemic. It is that complication of the infection that the vaccine is and always was intended to help mitigate.
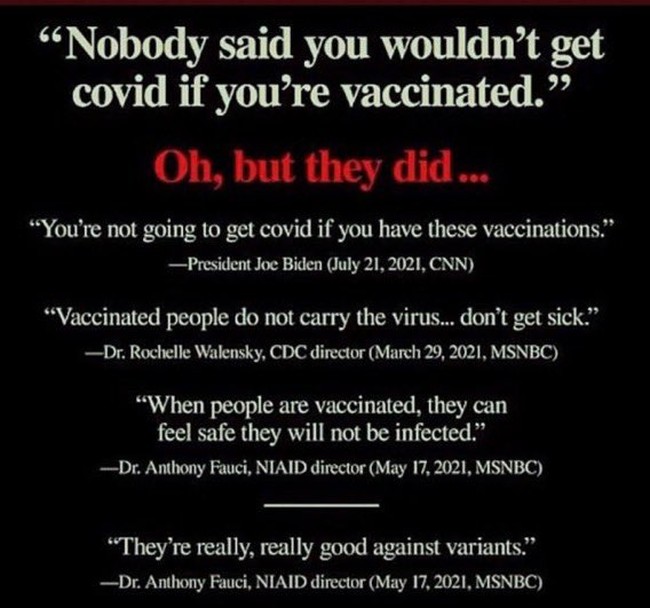
Ah. That’s not what they said until people kept on getting COVID after vaccinations. Then they fessed up.
How many times were you told that if you get vaccinated you wouldn’t get COVID? How many times did the vaccine promoters and mandators demand your vaccination to “protect others?” They always knew it was a lie. At least that is the case for the people like Fauci and Walensky.
As of 2022, after more than 60 years of experience with influenza vaccines, very little improvement in vaccine prevention of infection has been noted. As pointed out decades ago, and still true today, the rates of effectiveness of our best approved influenza vaccines would be inadequate for licensure for most other vaccine-preventable diseases.7 Even decades-long efforts to develop better, so-called “universal” influenza vaccines—vaccines that would create more broadly protective immunity, preferably lasting over longer time periods8,10—have not yet resulted in next-generation, broadly protective vaccines, although a large number of experimental vaccines are in preclinical or early clinical development.11
During the COVID-19 pandemic, the rapid development and deployment of SARS-CoV-2 vaccines has saved innumerable lives and helped to achieve early partial pandemic control.12 However, as variant SARS-CoV-2 strains have emerged, deficiencies in these vaccines reminiscent of influenza vaccines have become apparent. The vaccines for these two very different viruses have common characteristics: they elicit incomplete and short-lived protection against evolving virus variants that escape population immunity
We still haven’t gotten to the best parts of the paper, but already we are learning things that we haven’t been told. Gee, who told you that flu vaccines probably wouldn’t be eligible for licensure if they weren’t treated specially? Not my doctor. Not all those ads promoting the vaccine.
That seems like a bit of data that would have been nice to know.
Vaccines that work are different than those for respiratory viruses–and the flu and COVID vaccines have benefited from conflating the effective vaccines from those directed at respiratory viruses.
More than 50 years ago, the development of successful vaccines against some of the most important respiratory viruses, including measles, mumps, and rubella, led to the hope that vaccines could soon be developed for all other respiratory viruses. However, natural infections with these three vaccine-controlled respiratory viruses, as well as smallpox and varicella zoster virus (VZV), are not representative of infections caused by most respiratory viruses. They differ in at least three critically important ways that are related to their successful control with vaccines (Table 1):
What distinguishes these viruses from the respiratory ones is that they become problematic once they enter the body’s internal systems. Since that is the case, systemic vaccines work. Respiratory viruses rarely systemically infect people, so systemic vaccines never get a chance to work.
In stark contrast, the non-systemic respiratory viruses such as influenza viruses, SARS-CoV-2, and RSV tend to have significantly shorter incubation periods (Table 1) and rapid courses of viral replication. They replicate predominantly in local mucosal tissue, without causing viremia, and do not significantly encounter the systemic immune system or the full force of adaptive immune responses, which take at least 5–7 days to mature, usually well after the peak of viral replication and onward transmission to others. SARS-CoV-2 “RNAemia” (circulation of viral RNA in the bloodstream, as is seen with most mucosal respiratory virus infections, as distinct from viremia, in which infectious viruses can be cultured from the blood), has been reported, and RT-PCR levels of viral RNA have been linked to severe disease,23,24 similar to studies of influenza RNAemia.25,26 As a result, the non-systemically replicating respiratory viruses, apparently including SARS-CoV-2,13,14,15 tend to repeatedly re-infect people over their lifetimes without ever eliciting complete and durable protection.27
Do you see what he is saying here? No systemic vaccine for respiratory infections does or even can work to prevent infection and transmission of the viruses to others, because they never get a chance to. Everything important takes place in the mucosal system, which has a different immune response than the rest of the body.
Attempting to control mucosal respiratory viruses with systemically administered non-replicating vaccines has thus far been largely unsuccessful, indicating that new approaches are needed.
Gee whiz. That’s not what I remember being told.
I remember being told that if I don’t get the vaccine I will be Typhoid Mary, killing countless others. Grandma will die because of me.
The whole point of Fauci et. al.’s article in Cell is that we need a new kind of vaccine. Ones that will work.
Surely that would be nice. I am all for it. But let’s get back to the fact that you lied to everybody and caused the nastiest divisions in the country in decades.
Vaccine mandates were predicated on a lie–and a lie that Fauci and others KNEW was a lie. It’s not like they didn’t know the science. They simply lied about it. They censored people who told the truth. They forced millions to take an experimental drug with no studies on long-term medical complications. They got people fired, canceled, and destroyed based upon a claim that was false.
It is a scandal. And for the first time since this all began I am on board with tossing the man in jail. He committed massive fraud and medical malpractice and should pay a price.






Join the conversation as a VIP Member