
If you’re wondering why the Dow is up 700 points this morning, this is a big part of it. Any bit of meaningful incremental progress towards digging us out of the multitrillion-dollar economic hole we’re in is enough to unleash some “animal spirits.”
I’m going to go ahead and guess that this is the mystery data Moncef Slaoui alluded to at Friday’s White House press conference when he said he’d seen something lately that made him optimistic about having a vaccine by the end of the year. Slaoui is a member of Moderna’s board. Presumably he learned of these phase one results before most of the rest of the world did.
What’s especially interesting about Moderna’s progress is that the science here is innovative. They’re not working on a traditional vaccine in which the virus itself is rendered inactive and then injected into subjects to produce antibodies. They’re using a novel process based on mRNA, which raises the stakes for their trials. Will it even work? As importantly, will it work as well as, or better than, the traditional approach?
So far, so good. Although they’re not very far in the process.
Immunogenicity data are currently available for the 25 µg and 100 µg dose level (ages 18-55) after two doses (day 43) and at the 250 µg level (ages 18-55) after one dose (day 29). Dose dependent increases in immunogenicity were seen across the three dose levels, and between prime and boost within the 25 µg and 100 µg dose levels. All participants ages 18-55 (n=15 per cohort) across all three dose levels seroconverted by day 15 after a single dose. At day 43, two weeks following the second dose, at the 25 µg dose level (n=15), levels of binding antibodies were at the levels seen in convalescent sera (blood samples from people who have recovered from COVID-19) tested in the same assay. At day 43, at the 100 µg dose level (n=10), levels of binding antibodies significantly exceeded the levels seen in convalescent sera. Samples are not yet available for remaining participants.
At this time, neutralizing antibody data are available only for the first four participants in each of the 25 µg and 100 µg dose level cohorts. Consistent with the binding antibody data, mRNA-1273 vaccination elicited neutralizing antibodies in all eight of these participants, as measured by plaque reduction neutralization (PRNT) assays against live SARS-CoV-2. The levels of neutralizing antibodies at day 43 were at or above levels generally seen in convalescent sera.
Two key questions loom over phase one trials, as I understand it. One, obviously, is whether the vaccine works to produce antibodies. Moderna’s sample is small but the preliminary data says yes — the mRNA vaccine elicits as many antibodies, and at some doses even more antibodies, as actual infection from the coronavirus does. And it did prevent viral replication in the lungs of mice, per a separate study.
The second question is whether the vaccine causes side effects. The results here depended on the dose, with nothing more than a little redness at the point of injection for subjects who got the 25 µg and 100 µg shot. Three patients who got the big 250 µg experienced fever, headaches, and muscle aches for a day and then felt better. But we don’t need to worry much about the 250 µg dose: Because the lower doses worked fine, Moderna’s not planning to test the highest dose in later trials. Partly that’s a matter of wanting to limit side effects, I take it, and partly to stretch their stockpile of the virus further. It’d be fantastic if we can bring immunity to 10 people at the low dose instead of one person at the high one. “If you get to the level of [antibodies of] people who have had disease, that should be enough,” said the company’s chief medical officer.
Whether the antibodies generated by the vaccine actually work to protect subjects from COVID-19 is unclear right now. That’s what phase two of the trials is for. But scientists have been bullish on mRNA vaccines despite their novelty. The science is above my pay grade but this paper in Nature magazine from two years ago identifies several advantages to them over traditional vaccines, one of which is highly relevant in our current dystopian predicament.
The use of mRNA has several beneficial features over subunit, killed and live attenuated virus, as well as DNA-based vaccines. First, safety: as mRNA is a non-infectious, non-integrating platform, there is no potential risk of infection or insertional mutagenesis. Additionally, mRNA is degraded by normal cellular processes, and its in vivo half-life can be regulated through the use of various modifications and delivery methods. The inherent immunogenicity of the mRNA can be down-modulated to further increase the safety profile. Second, efficacy: various modifications make mRNA more stable and highly translatable. Efficient in vivo delivery can be achieved by formulating mRNA into carrier molecules, allowing rapid uptake and expression in the cytoplasm (reviewed in Refs 10,11). mRNA is the minimal genetic vector; therefore, anti-vector immunity is avoided, and mRNA vaccines can be administered repeatedly. Third, production: mRNA vaccines have the potential for rapid, inexpensive and scalable manufacturing, mainly owing to the high yields of in vitro transcription reactions.
If phases two and three go well, Moderna’s vaccine could be available for emergency use by the fall — although we shouldn’t get our hopes up. Describing Trump’s aim for a vaccine available at scale by year’s end, WaPo reported this weekend that “A number of senior administration officials said on the condition of anonymity that they are also skeptical of the president’s timeline but that Trump wanted to provide ‘hope.’ Birx has gently told the president it will be more difficult than he thinks to create a vaccine quickly.” Relatedly, read this skeptical take on Oxford’s promising early vaccine results from respected virologist William Haseltine. The Oxford vaccine may have prevented monkeys from getting sick, he notes, but it didn’t prevent them from being infected, suggesting a relatively weak immune effect. The titer of neutralizing antibodies produced by the vaccine was also relatively low compared to more traditional approaches.
This passage about the “adenovirus vector-based” model of Oxford’s vaccine caught my eye. Does it bode ill for Moderna’s vaccine?
What are the potential implications for other vaccine trials? We know adenovirus is a good vector for eliciting protective responses for protein coding genes of other viruses, in fact better than many others. This then raises the question of whether vaccine strategies based on the delivery of viral antigens by nucleic acids, be it DNA or RNA, will suffice. From the published data the nucleic acid of select viral genes and proteins delivery technology seems inferior to a whole killed virus vaccine approach.
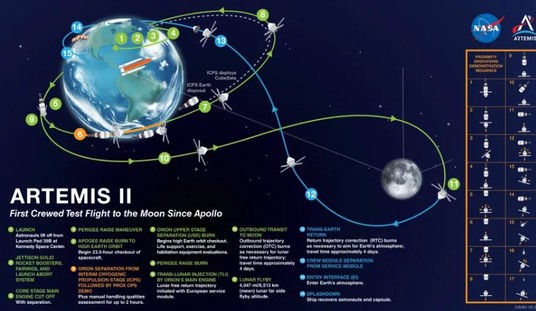
Various Chinese outfits are working on traditional whole-killed-virus vaccines. If Haseltine’s right, they may get to the moon before we do.
One more point to note about Moderna’s results. Subjects who received lower doses of the vaccine (25 µg and 100 µg) got two shots instead of one. At the lowest dose, it took until two weeks after the booster shot for subjects to have antibodies in their system in numbers equivalent to those seen in recovered coronavirus patients. Administering a single-dose vaccine to a population of 330 million people will be logistically challenging; administering a two-dose vaccine, with a booster required in the weeks after the first shot, would be that much more complicated. Moderna says it’s going to try a 50 µg dose in coming trials, though, which may solve this problem. They’re trying to find a sweet spot in a dose that’s high enough to be effective in one shot and low enough that it won’t produce side effects. Stay tuned.




Join the conversation as a VIP Member