First things first: there is no way to know for sure how common this is due to poor screening and reporting, but German researchers have decisively demonstrated through autopsy that the COVID-19 vaccine-induced myocarditis was the cause of death in 5 patients they autopsied after sudden deaths experienced shortly after COVID-19 vaccination.
The study was published in the peer reviewed journal Clinical Research in Cardiology. The doctor sharing the study is a Johns-Hopkins professor and graduate of the Harvard School of Public Health, so not a nobody in the public health world.
This is a German study from a reputable group. It's very hard to conduct this research in the U.S.
Germany also did the study showing that no healthy child 5-17 yrs of age died of Covid in that country. They also recommend against the Moderna vax in ppl <30. Not so with the CDC.
— Marty Makary MD, MPH (@MartyMakary) December 3, 2022
The study itself is very convincing, as it is based not upon a statistical analysis of deaths based upon ICD codes or anything like that. It is based entirely on autopsies conducted by the researchers themselves, all in a single hospital on patients who had experienced sudden deaths following shortly after COVID-19 vaccinations using mRNA vaccines. mRNA are apparently the vaccines likely to cause the adverse reactions.
They do no analysis of relative risk between COVID infection and vaccine reactions, and understandably so. It is essentially impossible to do that given that almost everybody has been infected by COVID at some point, but the precise numbers are unknown. Hence there is no definitive way to compare the relative risks, although it is known that COVID itself can cause myocarditis, as can other viral infections.
However, it is pretty clear that the risk is not insubstantial, given the fact that 5 patients were identified in a relatively short period of time at one hospital alone in Berlin. We cannot safely extrapolate from there to any particular number of cases in Germany or elsewhere, but the risk is obviously quite real. That is why Germany recommends against using the Moderna vaccine in anybody under 30. A precaution not made in the United States, where our public health officials are pushing the vaccine heavily and with no distinction between them.
Several interesting things came out of the study, including a few specific things that were unknown before. Among them is that they identified the mechanism causing the deaths, which mimics in miniature what COVID can do when it becomes life threatening.
Here are a few bits from the study, including the population studied and their conclusions.
Among the 35 cases of the University of Heidelberg, autopsies revealed other causes of death (due to pre-existing illnesses) in 10 patients (Supplementary Table 1). Hence, these were excluded from further analysis. Cardiac autopsy findings consistent with (epi-)myocarditis were found in five cases of the remaining 25 bodies found unexpectedly dead at home within 20 days following SARS-CoV-2 vaccination. Main characteristics of the five cases are presented in Table 2, while further autopsy findings are shown in Supplementary Table 2. Three of the deceased persons were women, two men. Median age at death was 58 years (range 46–75 years). Four persons died after the first vaccine jab, the remaining case after the second dose. All persons died within the first week following vaccination (mean 2.5 days, median 2 days).
You can already see one limitation of the study–in order to reduce the number of autopsies they would have to perform they screened the potential population of sudden deaths to study to patients who had just received the vaccine. Hence we have no idea whether the risks increase, decrease, or remain the same over time. They likely decrease, but we have no data from this study to back that up. It is an extrapolation made based upon the mechanism identified in the autopsies. Also their study was limited to myocarditis, leaving questions about whether risks from other causes might be worrisome.
Histological examination showed inflammatory infiltration of the myocardium. The infiltrate was focal and interstitial in all cases. It was predominantly detected in sections taken from the right ventricular wall and interventricular septum. The histological and immunohistochemical characterization revealed that the inflammatory infiltrate was predominantly composed of lymphocytes. … All cases lacked significant coronary heart disease, acute or chronic manifestations of ischaemic heart disease, manifestations of cardiomyopathy or other signs of a pre-existing, clinically relevant heart disease.
That is a long and fancy way of saying that the hearts were otherwise healthy, without any evidence of damage from prior injury or ischemic heart disease (which would cause a heart attack). What was found instead was an immunologic response that largely focused on the right ventricle, suggesting to them that blood coming into the heart was causing inflammation there specifically. They speculate that the vaccine was accidentally injected into a vein at a higher concentration than would occur from an intramuscular injection, and perhaps the spike protein caused too strong an immune response that damaged the heart muscle.
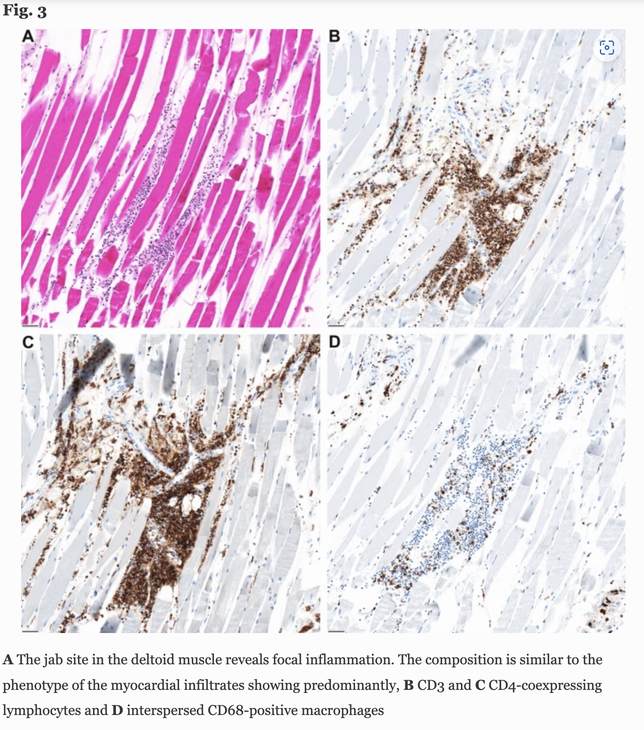
One thing that backs that theory up, although it fails to prove it, is the fact that the immune response in the heart mirrors what was found in the muscles around the injection site of a patient who died less than a day after injection.
Based on the autopsy findings and all available data, no other cause of death except (epi-)myocarditis was identified in any of the cases presented here. Hence, myocarditis has to be considered the likely cause of death. From a functional point of view, myocardial damage in our cases is not sufficient to postulate contractile failure as terminal cause of death; thus, arrhythmic failure, either by cardiac arrest or by ventricular fibrillation, has to be assumed as the mechanism leading to the patients’ death. Myocarditis-related acute cardiac arrest due to either asystoly or ventricular fibrillation is a well-established pathomechanism in other causes of acute myocarditis as well [22, 23].
Regarding the potential underlying pathogenesis of (epi-)myocarditis, our findings allow some considerations. Besides pneumonia, myocarditis is another manifestation reported during SARS-CoV-2-infection [24]. It is under debate whether myocarditis in COVID-19 is primarily caused by the viral infection or whether it occurs secondary as a consequence of the host´s immune response, in particular by T-lymphocyte-mediated cytotoxicity or as a consequence of the cytokine storm observed during COVID-19 [25]. Thus, it seems possible that a molecular mimicry between the spike protein of SARS-CoV-2 and self-antigens may trigger an anti-myocytic immune response in predisposed individuals. Multiple studies of mRNA-vaccines showed robust Receptor-Binding-Domain specific antibodies, T cell and cytokine responses [26]. T cells, especially CD4 + T cells, are the main drivers of heart-specific autoimmunity in myocarditis [27]. A vaccine-induced activation of the immune system in persons with otherwise peripheral tolerance due to regulatory T cells might promote CD4 + effector T cell expansion and myocarditis. Considering that (epi-)myocarditis has not been described following vector-based anti-SARS-CoV-2 immunization yet, it could also be possible that the immune response may be directed against the mRNA or other constituents of the vaccine formula. However, the vaccine against smallpox, based on a vaccinia virus, is reported to cause (epi-)myocarditis in rare cases [2, 3]. Of note, it has been recently reported that intravenous injection of COVID-19 mRNA vaccine is able to induce an acute (epi-) myocarditis in a preclinical model [28]. Interestingly, we recorded inflammatory foci predominantly in the right heart, which may suggest a gradual blood-stream derived dilution effect and based on this finding it is at least tempting to speculate that inadvertent intravascular vaccine injection may be contributive.
Breaking that out into English: the acute cause of death was almost certainly arrhythmia caused by damage to a specific area of the heart. The likely cause of that was focal damage, usually on the right side of the heart where the blood from the injection site would first appear. That is informed speculation.
Bottom line:
In general, a causal link between myocarditis and anti-SARS-CoV-2 vaccination is supported by several considerations: (A) a close temporal relation to vaccination; all cases were found dead within one week after vaccination, (B) absence of any other significant pre-existing heart disease, especially ischaemic heart disease or cardiomyopathy, (C) negative testing for potential myocarditis-causing infectious agents, (D) presence of a peculiar CD4 predominant T-cell infiltrate, suggesting an immune mediated mechanism. The latter criterion is supported by demonstration of a phenotypically identical T-cell infiltrate at the deltoidal injection site in one of the cases.
Does this all add up to “don’t get the COVID jab?” Not exactly. It all depends upon the relative risks for the people involved. COVID has its own risks, of course, and the vaccines we are told reduce the medical risks from COVID, although they clearly don’t prevent infection.
The study does seem to clearly show that mRNA vaccines are much more dangerous than advertised, and that we know far too little to treat them as if they were no more dangerous than saline solution. It also means, at least to me, that risk stratification is warranted when considering to whom the vaccine is given. A person with very little risk from a COVID infection–a young, healthy person with almost no risk of severe disease, should weigh the risks differently than an 80 year old with diabetes and heart disease.
That should be obvious to any sane person, but not, apparently, to our public health authorities who are going full speed ahead on trying to vaccinate everyone.
European countries have pulled back from their advocacy of vaccination, even limiting access to the vaccine for otherwise young and healthy people. In the US we are still suffering from a barrage of propaganda.
I have zero advice to give regarding whether anybody should get the vaccine. I am not a doctor, nor do I play one on TV. I got the first two jabs, and will get no more. I have decided that there just isn’t enough data to convince me that the risks are worth the payoff, and I have multiple comorbidities. My doctor also refrained from recommending it or recommending against it, because the CDC is simply too unreliable to trust.
What I will recommend is looking at the evidence yourself, or finding someone who can adequately understand the research to help you. As you can see, it takes a certain kind of mind to read and comprehend and a familiarity and comfort with the technical language. As a heart patient I dove into the medical research a long time ago so it doesn’t intimidate me any more. Find someone you trust and then think on it.
It’s your life, not theirs. Get the facts and make an informed decision.






Join the conversation as a VIP Member